What a Fertility Checkup Really Tells You
Most people don’t think about their fertility until they have a specific reason to. Whether you’re considering egg freezing, planning to start a family in the next few years, or simply curious about your reproductive health, a fertility checkup gives you concrete data before you need to act on it.
If something needs attention, you have time to address it. If everything looks normal, you have data to use as your baseline.
Getting a fertility checkup in your early 30s ensures that when you’re ready to make a move, you have the time and space to do it on your own terms.
What is a Fertility Checkup?
A fertility checkup isn’t the same as a standard gynecology visit or a well-woman exam. Your annual OB-GYN appointment doesn’t assess your ovarian reserve, and a Pap smear tells you nothing about your egg count or quality. These are entirely different tests that ask different questions about your body.
Sometimes called a fertility assessment or baseline workup, a fertility checkup is a targeted evaluation of your reproductive health. It combines bloodwork and a transvaginal ultrasound to check your ovarian reserve, looking at both your egg supply and whether anything in your hormonal profile warrants a closer look.
You don’t need a referral from your OB-GYN, and you don’t have to wait until you have a specific concern to schedule an appointment. It’s common to get a checkup simply because you’re planning for the future and want to know where you stand.
The Tests and What Each One Measures
The tests in a fertility workup vary depending on what you’re evaluating. If you’re considering egg freezing or fertility preservation, the core of your assessment focuses on ovarian reserve, specifically AMH and antral follicle count.
If you’re planning to try to conceive or pursue IVF, your provider will typically add a hormone panel to round out the testing. Here’s what each test covers.
For Egg Freezing and Fertility Preservation
AMH (Anti-Müllerian Hormone)
AMH is a hormone produced by the small follicles in your ovaries, making it the most reliable blood test for checking your ovarian reserve. Unlike other hormones, AMH stays relatively stable throughout your cycle, which means you can test on any day.
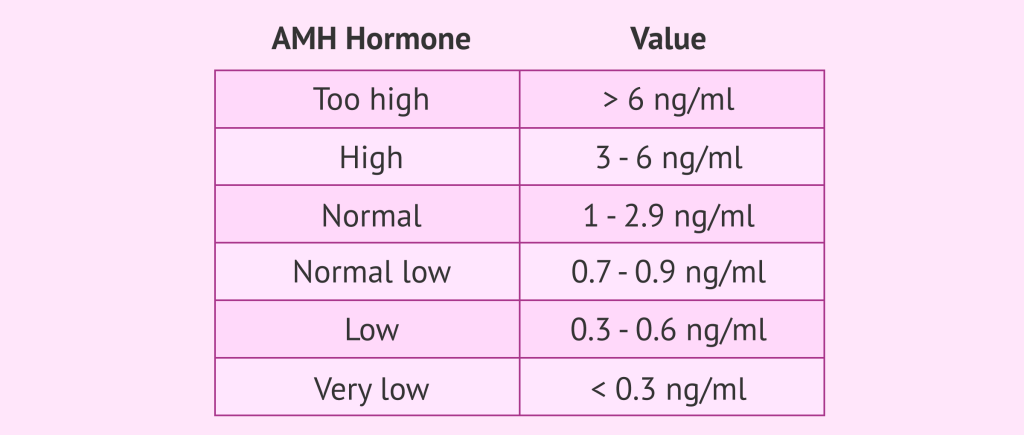
Higher levels suggest more follicles in reserve; lower levels point to a smaller pool. Looking at AMH alongside other results is what gives you a more complete and accurate picture of your fertility health.
AMH reference ranges vary by laboratory and assay. A result that reads as low by one lab’s standards may be interpreted differently using another assay. Your provider can put your numbers in context based on the specific lab used.
AFC (Antral Follicle Count)
Your antral follicle count is measured during a transvaginal ultrasound, usually on days 2 or 3 of your cycle. The sonographer counts the small, fluid-filled follicles in your ovaries. These are the follicles that have the potential to mature and release an egg that month.
Unlike AMH, AFC is a real-time snapshot rather than a stable marker; it can fluctuate from cycle to cycle and varies depending on who’s reading the scan. At Extend, AMH combined with age is the primary basis for assessing ovarian reserve.
For Those Planning to Conceive or Pursue IVF
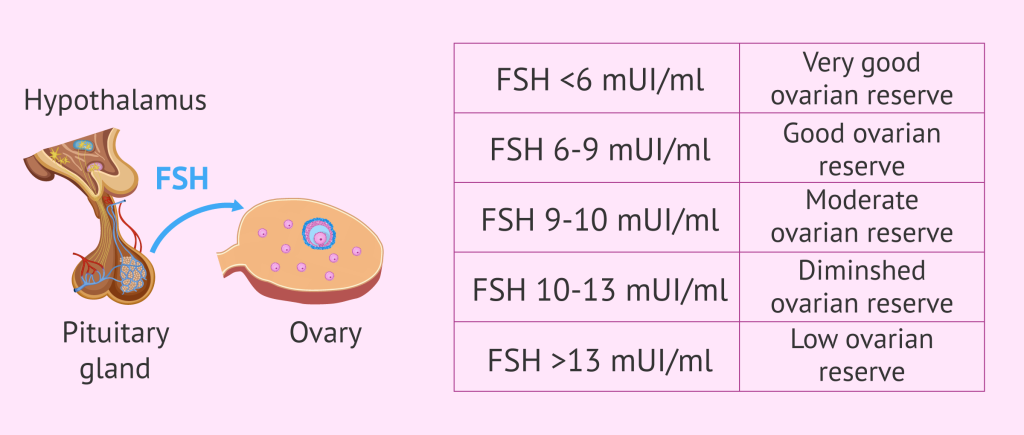
Day 3 FSH and Estradiol
FSH (follicle-stimulating hormone) is the signal your brain sends to get follicles growing at the start of each cycle. An elevated Day 3 FSH suggests your body is working harder than usual to stimulate the ovaries, which can be a sign of a lower reserve.
Estradiol is measured at the same time because high estradiol can artificially suppress your FSH, making it look normal when it isn’t. You need both numbers together to understand what’s happening.
Since these blood tests occur on day 2, 3, or 4 of your cycle, they take a bit of scheduling. Even with the extra logistics, they’re still a foundational part of a full fertility assessment.
Thyroid Function (TSH) and Prolactin
Neither of these tests measures ovarian reserve, but both are included in a fertility workup for a reason. Untreated thyroid disorders, including subclinical hypothyroidism, can lead to a higher chance of infertility and pregnancy issues.
Similarly, elevated prolactin can disrupt ovulation and throw off cycle regularity. Both conditions are treatable; the point of screening is to catch them before you’re trying to conceive, not after.
What the Results Tell You and What They Don’t
A fertility checkup doesn’t tell you whether you’ll get pregnant or how long it will take. A normal AMH does not guarantee fertility, and a low AMH doesn’t mean you can’t conceive. These tests measure what’s measurable—ovarian reserve and hormonal function. But the reality is that fertility involves more variables than any single hormone panel can capture.
For someone with a low AMH in their early 30s, that information can inspire action. They might decide to freeze eggs now rather than waiting, move up their timeline to try to conceive, or consult a reproductive endocrinologist before their options narrow. Without the data, none of that is possible.
Many people with a lower ovarian reserve can still get pregnant without intervention. But it’s worth having a proactive conversation with a specialist before the need is urgent.
Why Your Early 30s Are the Right Time to Check In
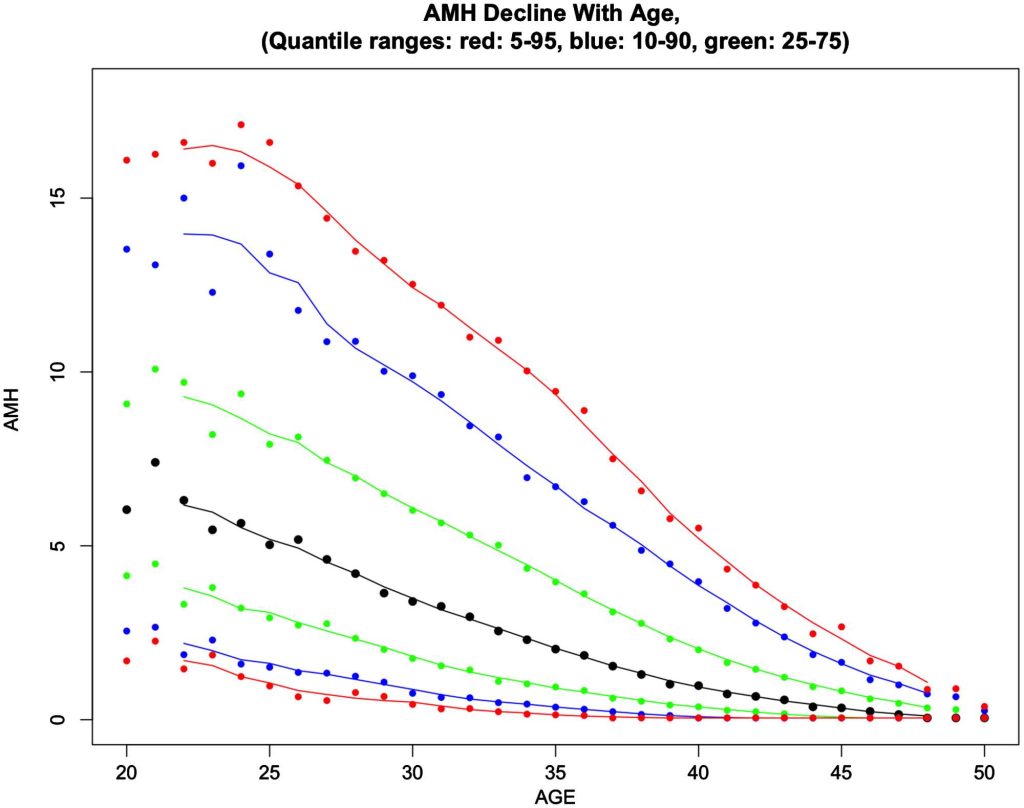
The conventional wisdom tells us to wait until 35 to start thinking about fertility. But by then, your ovarian reserve has already been declining for years.
Having a baseline in your early 30s—or even your late 20s if you have a family history of early menopause, endometriosis, or PMOS (Polyendocrine Metabolic Ovarian Syndrome, formerly PCOS)—helps you avoid starting from scratch at 35 or 36. You have a reference point, and if something is off, you have time to act on it.
Between 30 and 35, AMH declines more steeply than it did in your 20s. Egg quality, which no blood test can currently measure, begins to shift more noticeably in your early to mid-30s. Your FSH levels may start to climb as the ovaries need stronger stimulation. But this isn’t a reason to panic. It just makes a strong case for knowing where you are before those changes accelerate.
What to Do with the Information
If your results come back within normal range for your age, your baseline is established. That doesn’t mean you can put fertility out of your mind forever, but it does mean you’re not facing immediate pressure. Your provider can walk you through what “normal” truly means for your age, health history, and reproductive goals.
If something is off, like a low AMH or an elevated FSH, that warrants a conversation with a reproductive endocrinologist. Understanding your options, with plenty of time to weigh them, is why early testing is so important.
Egg freezing, if it’s something you’re considering, is most effective when done earlier in your 30s. Mature eggs are retrieved during the freezing process, and both the number and quality of those eggs are usually higher at 31 than at 37. A fertility checkup is often the first step in egg freezing, giving you and your provider the baseline information you need to plan for your future.
The Takeaway
A fertility checkup won’t tell you everything. It won’t predict if or when you’ll get pregnant, and it won’t make decisions for you. But it does give you all the facts when you can still make sense of them.
If you’re in your late 20s or early 30s and haven’t had a fertility assessment, it’s a smart and proactive move. Getting a head start now is a luxury that allows you to think and plan.
If you’re ready, a fertility checkup is the place to start. Extend’s fertility advisors can answer your questions and schedule your workup. Book a consultation today.
The post What a Fertility Checkup Really Tells You appeared first on Extend Fertility.