What Ovarian Reserve Has (and Doesn’t Have) to Do with Ovarian Cancer
Ovarian cancer brings up many heavy questions about fertility. Since the ovaries house your egg supply, the diagnosis and treatment are often at odds. It’s usually the treatment that poses the biggest risk; chemotherapy and radiation can take a toll on ovarian function.
But there are paths forward. Depending on the stage, you might be a candidate for fertility-sparing surgery or have the option to pursue preservation before starting treatment.
What Ovarian Reserve Measures
Think of your ovarian reserve as a snapshot of your current egg supply. It’s something that changes naturally over time, though health conditions or past surgeries can speed up the process.
Clinicians typically use a combination of blood work (AMH and FSH) and an ultrasound (AFC) to get the full picture. These numbers are tools that help you and your doctor plan the best path forward for fertility treatment. Even if the numbers are low, pregnancy is still possible; they just help you understand which options to focus on and how quickly you may need to move.
Ovarian Cancer Is No Longer Primarily a Disease of Older Women
For a long time, the conversation around ovarian cancer focused almost entirely on older women. But that framing is outdated. Newer studies show that while cases in women over 50 are going down, the numbers for those under 50 are climbing. It’s a pattern researchers are still trying to explain, but it’s happening globally.
Overall cancer rates in women under 50 are now 82% higher than in men of the same age group—up from 51% in 2002. While ovarian cancer is still rare, the American Cancer Society expects 21,010 new diagnoses in 2026. For anyone in their 20s or 30s thinking about starting a family someday, the fertility planning conversation is now more urgent.
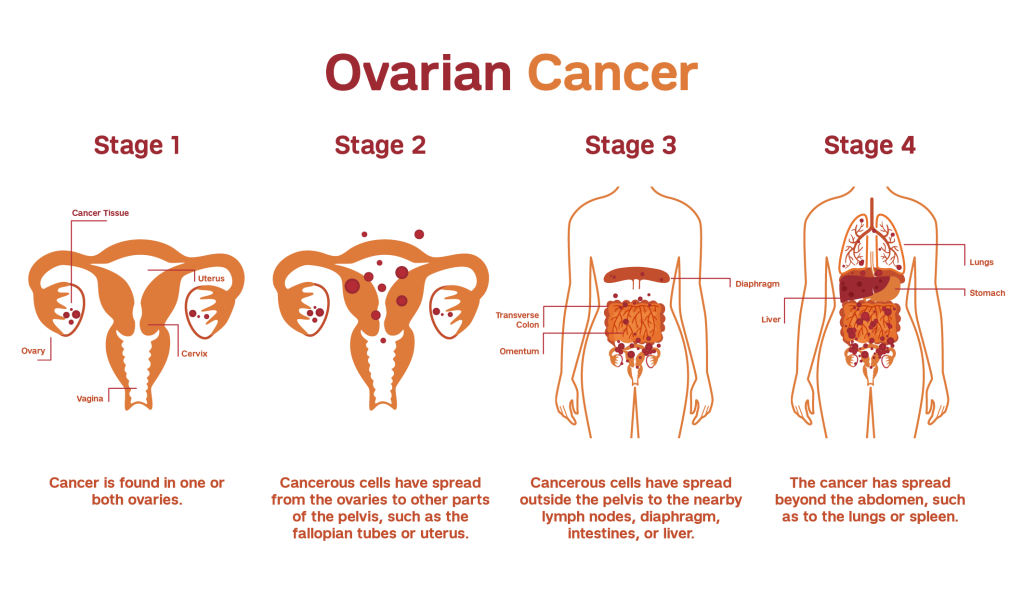
How Ovarian Cancer Affects the Ovaries
The ovaries have two major jobs: they balance your hormones and protect your lifetime supply of eggs. Since ovarian cancer begins in the ovaries, which hold your egg supply, a diagnosis immediately impacts your reproductive health. If the cancer is limited to one ovary, the health of your remaining ovary and the intensity of your treatment influence your future options.
Different tumor types, like germ cell or epithelial, require separate treatment approaches. For example, cancer caught early in one ovary is very different from a more advanced case. If it’s safe to do so, many women consider fertility-sparing surgery, which preserves the healthy ovary and uterus. It’s not the right fit for every diagnosis, but it’s an important conversation to have with your care team.
Planning for life after your diagnosis is a conversation worth having before you begin treatment. For some women, that conversation starts early. If you carry a BRCA1 or BRCA2 mutation, your lifetime risk increases significantly—up to 44% for BRCA1 and 17% for BRCA2, compared to just 1-2% for most people. Given the odds, many women eventually choose a prophylactic salpingo-oophorectomy, or surgery to remove their ovaries and tubes. This surgery completely removes your ovarian reserve, making timing even more critical.
What Cancer Treatment Does to Ovarian Reserve
Even if the cancer hasn’t touched your ovarian function, the treatment is often the biggest risk. Many chemotherapy and radiation treatments are ‘gonadotoxic,’ meaning they can damage ovarian tissue and eggs, sometimes for good.
The standard chemotherapy for the most common types of ovarian cancer usually combines a platinum-based drug with a taxane (a potent chemotherapy drug). Both are known to be tough on your egg supply. When you add radiation or bone marrow transplants into the mix, the risk of Premature Ovarian Insufficiency (POI)—where your ovaries stop working before age 40—ranges from 92 to 100%.
Since POI is often permanent, the window to protect your fertility is before treatment begins, not once it’s already underway.
Fertility Preservation for Ovarian Cancer: Options and Timing
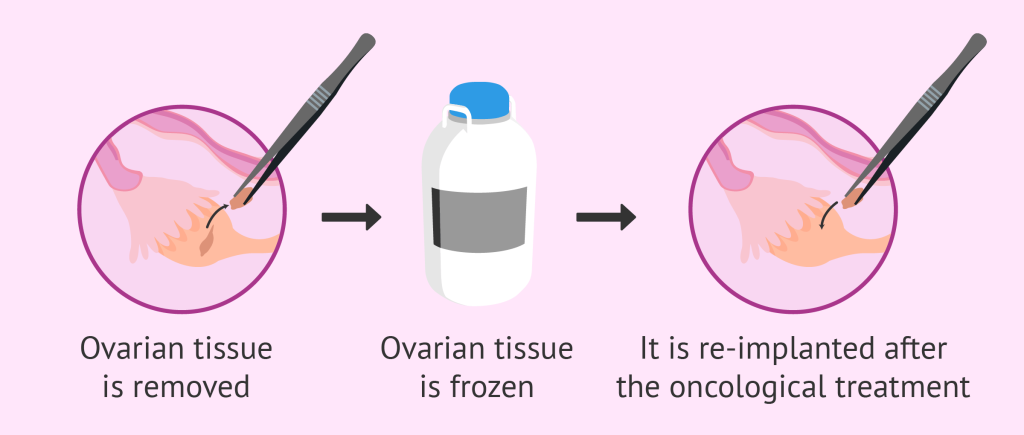
Fertility preservation is a standard part of cancer care today, but the right option depends on your timeline. Generally, there are three main paths: egg freezing, embryo freezing, and ovarian tissue freezing.
If you have about two weeks before treatment starts, egg or embryo freezing is usually the go-to option. It involves 10-14 days of stimulation to retrieve mature eggs. However, if your treatment is too urgent to wait for a full stimulation cycle, ovarian tissue freezing is a newer option. This involves surgically removing and freezing tissue to potentially reimplant later.
Deciding which path to take is a personal process. It involves looking at your current egg reserve, your cancer stage, and whether you’re planning to use a partner or donor sperm. This is why providers recommend a baseline fertility assessment; it documents your current fertility status so you can monitor your health post-treatment.
Research shows that talking to a reproductive specialist, not just your oncologist, leads to a much higher quality of life later on. You’ll feel more confident in your decision and have far less regret down the road.
If You Haven’t Had a Diagnosis
Most people reading this aren’t facing a diagnosis. You might be here because you’re thinking about freezing your eggs, looking into your family history, or just wanting to understand your fertility baseline. Whatever the reason, knowing your ovarian reserve gives you a head start.
An AMH test is a simple blood draw. While it won’t predict a cancer diagnosis, it gives you an idea of where your egg supply stands today. It’s always better to have the answers to those questions now while your options are open.
Ovarian cancer itself doesn’t always affect your eggs, but the treatment almost always does. If you’ve received a diagnosis, bring up fertility immediately with your provider. Whether it’s fertility-sparing surgery or freezing eggs, these steps are most effective before your treatment begins.
If you’re healthy, the same principle applies: knowing your baseline now keeps your options open later on.
If this post brought up questions about your own fertility, come talk to one of our fertility specialists. We’re here to help you explore your fertility preservation options.
The post What Ovarian Reserve Has (and Doesn’t Have) to Do with Ovarian Cancer appeared first on Extend Fertility.